 “I’m Home!” Every patient wants to return home with these words—day after
day. Every patient hopes medication or hospitalization will cure his or her
illness.
“I’m Home!” Every patient wants to return home with these words—day after
day. Every patient hopes medication or hospitalization will cure his or her
illness.
Researchers develop medicine, which doctors use to treat patients. Each patient
tries hard to get better. However, there are still diseases that medicine cannot
cure. “Childhood cancer" is one of them and develops in approximately 2000 to
3000 children every year in Japan. While the accurate number is unknown, 10,000
to 15,000 children are estimated to be in treatment for cancer. According to the
Registration of Vital Statistics in 2005, the estimated number of deaths due to
childhood cancer is approximately 100 to 150 children per 100,000 children. The
Registration shows that the estimated mortality rate for childhood cancer is
decreasing.
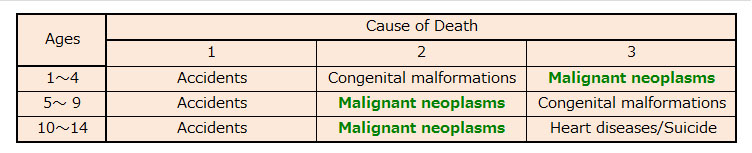
However, childhood cancer still has a high mortality rate and “malignant
neoplasm” is ranked one of the highest causes for childhood deaths in Japan.
(See Table). Of the three highest-ranked causes of childhood deaths, the only
cause that can be cured by medication is “malignant neoplasm.” However, there
still is no effective therapeutic medicine which can cure 100% of childhood
cancers. There is no preventive medicine, either.
|
Rank: Cause of Death in Children
|
|
|
(2005 Vital Statistics)
|
The mortality rate for childhood cancer is decreasing. However, because the
mechanism of pathogenesis on childhood cancer still remains largely unknown
despite medical advancements in recent years, the estimated morbidity rate for
childhood cancer has not improved.
In developing therapeutic medicine for childhood cancer, the safety and
effectiveness of the medicine must be first confirmed by statistical data
through clinical trial. Prior to conducting clinical trial, a “protocol” that
sets forth the objective and other details of the trial is prepared. Among other
things, a protocol will designate the number of participants necessary to
produce statistically significant data after considering the safety and
effectiveness of the medicine against the incident rate of a subject disease.
Even though childhood cancer is the second highest ranked cause of death of
children, the number of childhood cancer patients is still small and many young
patients do not qualify for the study because many drugs are proven safe only
for adult use or researchers are unable to administer sufficient amounts of
drugs into these patients. Further, childhood cancer is a generic classification
for cancer in children. In fact, childhood cancer has twelve major types, which
are further categorized into forty-seven subtypes of cancer (ICCC-3 third Ed.).
Therefore, if a clinical study was performed for a potential new drug or
therapy, the clinical study may not be supported by a statistically significant
volume of data because fewer subjects are available for these study criteria.
Due to Japan’s declining birthrate, the population of young children and
consequently the number of childhood cancer patients have decreased. Therefore,
the development of new drugs for childhood cancer is expected to be more
difficult in the future. Despite these difficulties, we hope we can help
develop a new effective childhood cancer drug and therapeutic cure for childhood
cancer!
|